A Patient's Guide to Lumbar Degenerative Disc Disease

Introduction
The intervertebral discs in the lower spine are commonly blamed for low back pain. Yet low back pain has many possible causes, and doctors aren't always certain why symptoms occur.
During an office visit for low back pain, your doctor may describe how changes in the discs can lead to back pain. When talking about these changes, your doctor may use the terms "degeneration" or "degenerative disc disease." Although the parts of the spine do change with time and in some sense degenerate, this does not mean a person's spine is deteriorating and that he or she is headed for future pain and problems. These terms are simply a starting point for describing what occurs in the spine over time and how the changes may explain the symptoms people feel.
This guide will help you understand
- how degenerative disc disease develops
- how doctors diagnose the condition
- what treatment options are available
Chiropractic Treatment
Low back pain is the number one reason patients seek care at the Winchester Hospital Chiropractic Center. We see hundreds of patients a week for this condition alone. Manual treatments such as spinal manipulation have been shown to be the most effective in treating people with lower back pain. Chiropractic doctors are the experts in spinal adjustments and manipulation. In fact, chiropractors perform 94% of all spinal manipulations in the United States. Spinal manipulation is one of the only ways to induce motion at specific vertebra in the spine. Chiropractic adjustments help restore normal motion to the joints, reduce pain and inflammation and relieve irritation to the sensitive nerves. Additionally, you will also be shown neutral spinal postures aimed at decreasing pain, improving mobility, strength and function. Patients are taught how to protect their spines and prevent the problems from returning again. Strengthening exercises are also incorporated. Treatments are often combined with electrical muscle stimulation, ice, ultrasound, exercises, exercise balls, soft tissue massage, and traction. All of these are designed to help decrease pain and inflammation and improve function and mobility. Nutritional recommendations may be prescribed. For example, glucosamine sulfate has been proven effective in not only reducing pain, but in reversing some of the wear in cartilage and actually stimulating new growth of the cartilage. Ginger extract has been shown to have the same clinical effects on pain as does Celebrex.
Anatomy
What parts of the spine are involved?
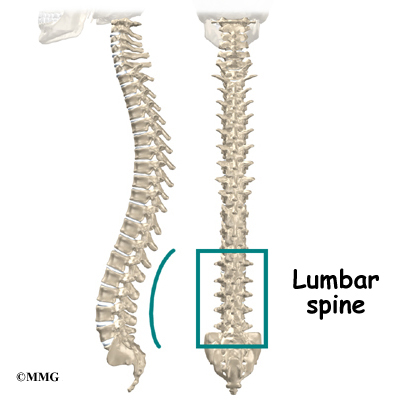
The human spine is made up of twenty-four spinal bones, called vertebrae. Vertebrae are stacked on top of one another to form the spinal column. The spinal column gives the body its form. It is the body's main upright support. The section of the spine in the lower back is known as the lumbar spine.
An intervertebral disc sits between each pair of vertebrae. The intervertebral disc is made of connective tissue. Connective tissue is the material that holds the living cells of the body together. Most connective tissue is made of fibers of a material called collagen. These fibers help the disc withstand tension and pressure.
The disc normally works like a shock absorber. It protects the spine against the daily pull of gravity. It also protects the spine during strenuous activities that put strong force on the spine, such as jumping, running, and lifting.
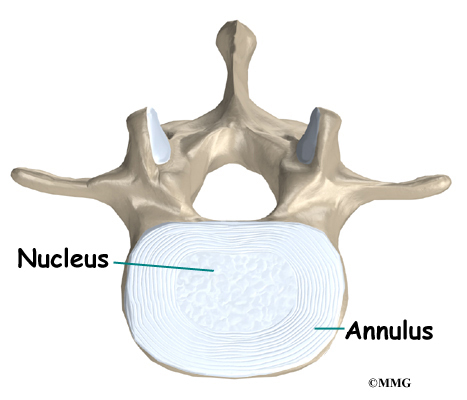
An intervertebral disc is made of two parts. The center, called the nucleus, is spongy. It provides most of the disc's ability to absorb shock. The nucleus is held in place by the annulus, a series of strong ligament rings surrounding it. Ligaments are connective tissues that attach bones to other bones.
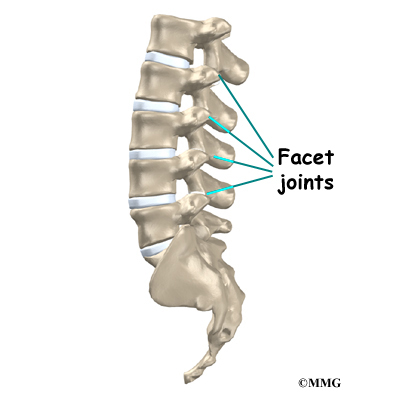
Between the vertebrae of each spinal segment are two facet joints. The facet joints are located on the back of the spinal column. There are two facet joints between each pair of vertebrae--one on each side of the spine. A facet joint is made of small, bony knobs that line up along the back of the spine. Where these knobs meet, they form a joint that connects the two vertebrae. The alignment of the facet joints of the lumbar spine allows freedom of movement as you bend forward and back.
Causes
Why do I have this problem?
Our intervertebral discs change with age, much like our hair turns gray. Conditions such as a major back injury or fracture can affect how the spine works, making the changes happen even faster. Daily wear and tear and certain types of vibration can also speed up degeneration in the spine. In addition, strong evidence suggests that smoking speeds up degeneration of the spine. Scientists have also found links among family members, showing that genetics plays a role in how fast these changes occur.
Disc degeneration follows a predictable pattern. First, the nucleus in the center of the disc begins to lose its ability to absorb water. The disc becomes dehydrated. Then the nucleus becomes thick and fibrous, so that it looks much the same as the annulus. As a result, the nucleus isn't able to absorb shock as well. Routine stress and strain begin to take a toll on the structures of the spine. Tears form around the annulus. The disc weakens. It starts to collapse, and the bones of the spine compress.
View animation of degeneration
This degeneration does not always mean the disc becomes a source of pain. In fact, X-rays and MRI scans show that people with severe disc degeneration don't always feel pain.

Pain caused by degenerative disc disease is mainly mechanical pain, meaning it comes from the parts of the spine that move during activity--the discs, ligaments, and facet joints. Movement within the weakened structures of the spine causes them to become irritated and painful.
Symptoms
What does the condition feel like?
Pain in the center of the low back is often the first symptom patients feel. It usually starts to affect patients in their twenties and thirties. Pain tends to worsen after heavy physical activity or staying in one posture for a long time. The back may also begin to feel stiff. Resting the back eases pain. At first, symptoms only last a few days.
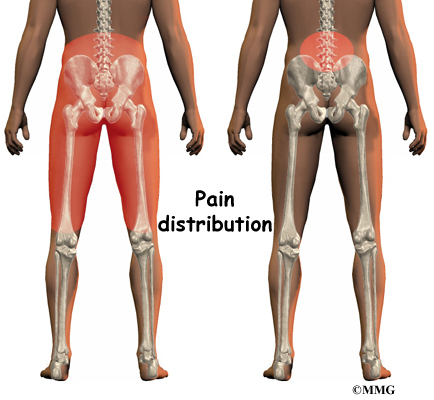
This type of back pain often comes and goes over the years. Doctors call this recurring back pain. Each time it strikes, the pain may seem worse than the time before. Eventually the pain may spread into the buttocks or thighs, and it may take longer for the pain to subside.
Diagnosis
How do doctors diagnose the problem?
Diagnosis begins with a complete history and physical exam. Your doctor will ask questions about your symptoms and how your problem is affecting your daily activities. Your doctor will also want to know what positions or activities make your symptoms worse or better.
Then the doctor does a physical examination by checking your posture and the amount of movement in your low back. Your doctor checks to see which back movements cause pain or other symptoms. Your skin sensation, muscle strength, and reflexes are also tested.
Doctors rely on the history and physical exam to determine which treatments will help the most. X-rays are rarely ordered on the first doctor visit for this problem. This is because over 30 percent of low back X-rays show abnormalities from degeneration, even in people who aren't having symptoms.
However, if symptoms are severe and aren't going away, the doctor may order an X-ray. The test can show if one or more discs has started to collapse. It can also show if there are bone spurs in the vertebrae and facet joints. Bone spurs are small points of bone that form with degeneration.
When more information is needed, your doctor may order magnetic resonance imaging (MRI). The MRI machine uses magnetic waves rather than X-rays to show the soft tissues of the body. It is helpful for showing if the tissues in the disc are able to absorb water and whether there are cracks inside the disc. It can also show if there are problems in other soft tissues, such as the spinal nerves.
Discography can help with the diagnosis. This is a specialized X-ray test in which dye is injected into one or more discs. The dye is seen on X-ray and can give some information about the health of the disc or discs. This test may be done when the surgeon is considering surgery, since it can help determine which disc is causing the symptoms.
Treatment
What treatment options are available?
Surgery
People with degenerative disc problems tend to gradually improve over time. Most do not need surgery. In fact, only one to three percent of patients with degenerative disc problems typically require surgery.
Doctors prefer to try nonsurgical treatment for a minimum of three months before considering surgery. If after this period nonsurgical treatment hasn't improved symptoms, the doctor may recommend surgery. The main types of surgery for degenerative disc problems include
- lumbar laminectomy
- discectomy
- fusion
Lumbar Laminectomy
The lamina forms a roof-like structure over the back of the spinal column. When the nerves in the spinal canal are squeezed by a degenerated disc or by bone spurs pushing into the canal, a laminectomy removes part or all of the lamina to release pressure on the spinal nerves.
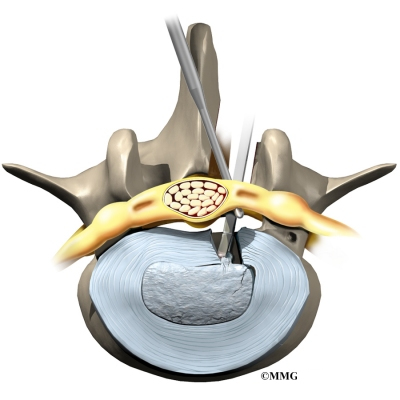
Discectomy
Surgery to take out part or all of a problem disc in the low back is called discectomy. Discectomy is done when the degenerated disc has ruptured (herniated) into the spinal canal, putting pressure on the spinal nerves. Surgeons generally perform this operation through an incision in the low back. Traditional methods involve chipping a small part of the lamina bone off the back of the spinal column. This is called laminotomy. It leaves greater room for the surgeon to remove the disc. Laminotomy differs from laminectomy (described above) in that laminectomy involves removing most or all of the lamina.
Many doctors now do procedures that require only small incisions in the low back. Categorized as "minimally invasive surgeries," these procedures are used to remove damaged portions of the problem disc. Advocates believe that this type of surgery is easier to perform. They also believe it prevents scarring around the nerves and joints and helps patients recover more quickly. Examples include percutaneous lumbar discectomy, laser discectomy, and microdiscectomy.
Fusion
Fusion surgery joins two or more bones into one solid bone. This prevents the bones and joints from moving. The procedure is sometimes done with a disc excision. Mechanical pain is eased because the fusion holds the moving parts steady, so they can't cause irritation and inflammation.
The main types of fusion for degenerative disc problems include
- anterior lumbar interbody fusion
- posterior lumbar fusion
- combined fusion
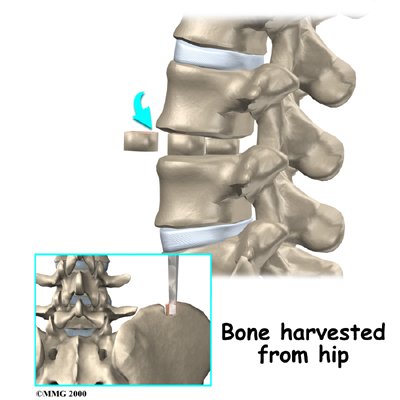
Anterior Lumbar Interbody Fusion
This surgery is done through the abdomen, allowing the doctor to work on the front (anterior) of the lumbar spine. Removing the disc (discectomy) leaves a space between the pair of vertebrae. This "interbody" space is filled with a bone graft. One method is to take a graft from the pelvic bone and tamp it into place. Another method involves inserting two hollow titanium screws packed with bone, called fusion cages, into the place where the disc was taken out. The bone graft inside the cages fuses with the adjacent vertebrae, forming one solid bone.
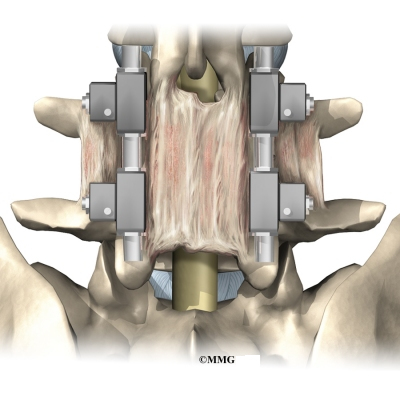
Posterior Lumbar Fusion
A posterior lumbar fusion is done though an incision in the back. In this procedure, the surgeon lays small grafts of bone over the problem vertebrae. Most surgeons will also apply metal plates and screws to hold the vertebrae in place while they heal. This protects the graft so it can heal better and faster.
Combined Fusion
As its name suggests, this procedure involves fusing the anterior (front) and posterior (back) surfaces of the problem vertebrae. By locking the vertebrae from the front and back, some doctors believe the graft stays solid and is prevented from collapsing. Results do show improved fusion of the graft, though patients seem to fare equally well with other methods of fusion.

All content provided by eORTHOPOD® is a registered trademark of Medical Multimedia Group, L.L.C.. Content is the sole property of Medical Multimedia Group, L.L.C.. and used herein by permission.
All materials from eORTHOPOD® are the sole property of Medical Multimedia Group, L.L.C.. and are used herein by permission. eORTHOPOD® is a registered trademark of Medical Multimedia Group, L.L.C..
|
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}